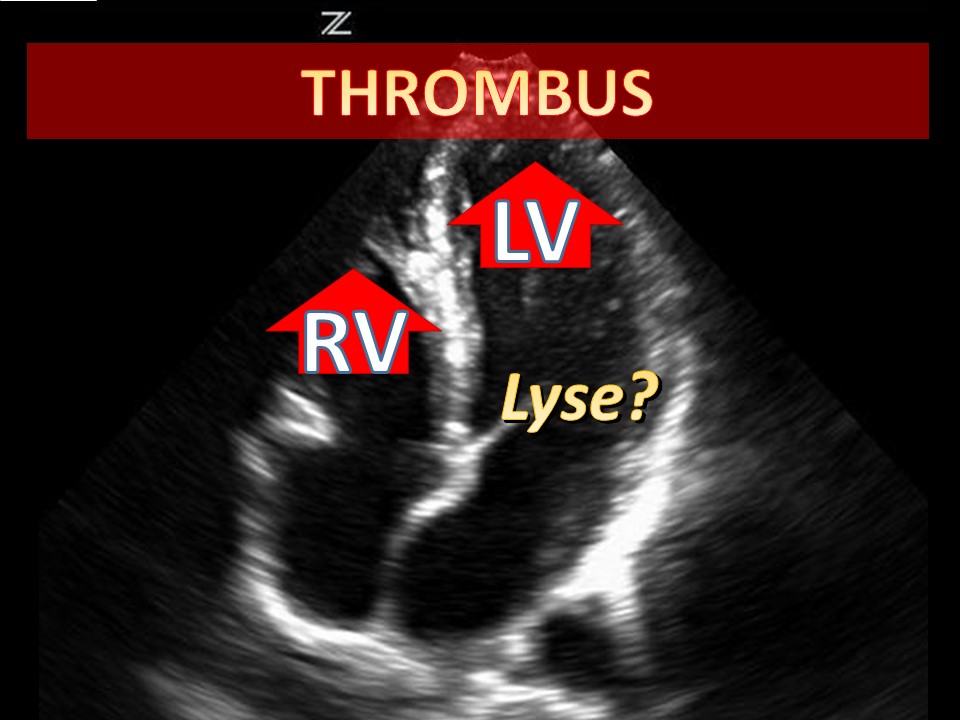
Your eyes may fool you...
Keep your differential diagnosis open.
Selected References
Barnard, et al. Rapid sequence induction of anaesthesia via the intraosseous route: a prospective observational study. Emerg Med J. 2014; Jun 24. pii: emermed-2014-203740.
Jousi M, Saikko S, Nurmi J. Intraosseous blood samples for point-of-care analysis: agreement between intraosseous and arterial analyses. Scand J Trauma Resusc Emerg Med. 2017;25(1):92. Published 2017 Sep 11. doi:10.1186/s13049-017-0435-4
Knuth, et al. Intraosseous Injection of Iodinated Computed Tomography Contrast Agent in an Adult Blunt Trauma Patient. Annals of Emergency Medicine. 2011; 57 (4) 382-386
Miller LJ. et al A new study of intraosseous blood for laboratory analysis.Arch Pathol Lab Med. 2010 Sep;134(9):1253-60.
Miller, et al. Utility of an intraosseous vascular system to deliver contrast dye using a power injector for computerized tomography studies. Annals of Emergency Medicine. 2011; 58 (4) 240-241.
Selected References
Aravindhan N, Chisholm DG. Sulfhemoglobinemia presenting as pulse oximetry desaturations. Anesthesiology. 2000;93:883–884.
So T-Y et al. Topical Benzocaine-induced Methemoglobinemia in the Pediatric Population. J Pediatr Health Care. 22(6):335–339.
Failure to Thrive (FTT) is not just for the clinics. We need to be on the lookout, because if we find it, there is already a big problem.
Definitions of Failure to Thrive may quibble on the details, but for us in the ED:
We can get around the longitudinal requirement by looking at weight as a "spot check" -- if grossly below weight without any other chronic condition, be alarmed.
Failure to thrive results from inadequate calories. This may be due to:
Any concern should trigger a more complete H&P (in audio).
Classic instructional video on the mother-infant dyad (scan through for various types).
After a focused H&P, you may need to admit the child for further workup, or to show that he can/cannot gain weight with routine care.
Remember, if you are the first one to bring this up, there is a real problem. By definition, an outpatient plan has failed. We will not be able to distinguish among the various possibilities of organic and non-organic causes (or mix thereof); our job is to be ready to catch it and act on it. The child's development, future intelligence, and welfare are at risk.
References
Birth to 24 months: Boys Weight-for-length percentiles and Head circumference-for-age percentiles
Birth to 24 months: Boys Length-for-age percentiles and Weight-for-age percentiles
Birth to 24 months: Girls Weight-for-length percentiles and Head circumference-for-age percentiles
Birth to 24 months: Girls Length-for-age percentiles and Weight-for-age percentiles
Jaffe AC. Failure to Thrive. Pediatrics in Review. 2011; 32(3)
Prutsky GJ et al. When Developmental Delay and Failure to Thrive Are Not Psychosocial. Hospital Pediatrics. 2016; (1):6
No one ever wants to find himself in this situation. A factory explodes. A building catches fire. A multi-vehicle traffic collision. Or an act of terrorism.
Very quickly, we have to scrap business as usual. We have to adapt to our new circumstances.
Definition of a mass casualty incident (MCI):
An incident which produces multiple casualties such that emergency services, medical personnel and referral systems within the normal catchment area cannot provide adequate and timely response and care without unacceptable mortality and/or morbidity.
In other words, our demand far outpaces our resources.
"If you can hear the sound of my voice, follow me". Those patients are GREEN, minor.
Otherwise, we need a system to distinguish those who can be DELAYED, IMMEDIATE, or EXPECTANT (soon to be deceased).
Use Simple Triage and Rapid Treatment (START) for 8 or older, JumpSTART for less than 8 years of age.

For Older Children, Adolescents, and Adults (8 or greater) -- START:
For Children less than 8 years of age (Infants Use Pediatric Assessment Triangle) -- JumpSTART:

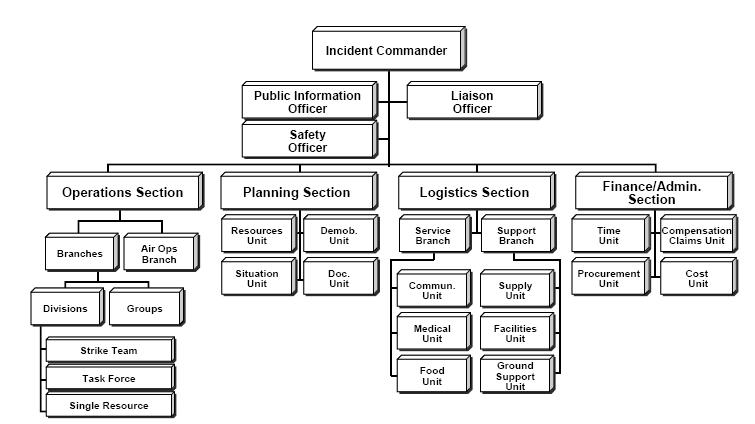 MCI Organizational Chart
MCI Organizational ChartSelected References
Briggs SM. Disaster management teams. Curr Opin Crit Care. 2005 Dec;11(6):585-
Culley JM, Svendsen E. A review of the literature on the validity of mass casualty triage systems with a focus on chemical exposures. American journal of disaster medicine. 2014; 9(2):137-150
FEMA IS 0100.b - Introduction to the Incident Command System (ICS), Student Manual. http://training.fema.gov/emiweb/is/is100b/student%20manual/02ics100b_sm_october2013.pdf. Accessed 03 MAY 2019.
Jensen J, Youngs G. Explaining implementation behaviour of the National Incident Management System (NIMS). Disasters. 2015 Apr;39(2):362-88. doi: 10.1111/disa.12103.
Lee JS, Franc JM. Impact of a Two-step Emergency Department Triage Model with START, then CTAS, on Patient Flow During a Simulated Mass-casualty Incident. Prehosp Disaster Med. 2015 Jun 24:1-7.
Lerner EB, Schwartz RB, Coule PL, et al. "Mass Casualty Triage: An Evaluation of the Data and Development of a Proposed National Guideline." Disaster Medicine and Public Health Preparedness 2(Suppl. 1) 2008, pp S25-S34.
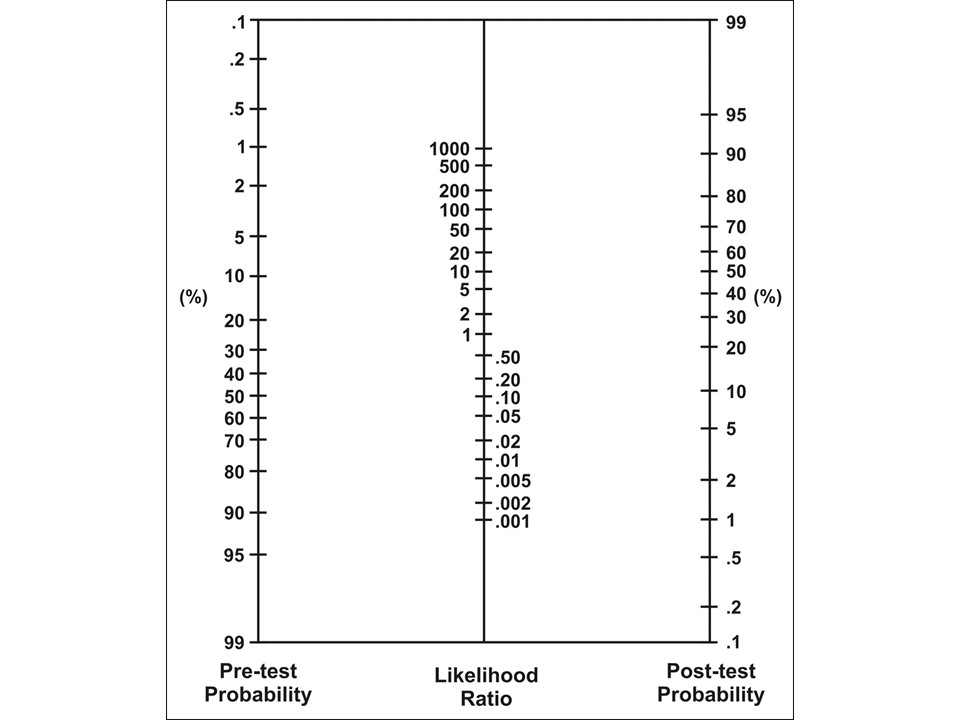
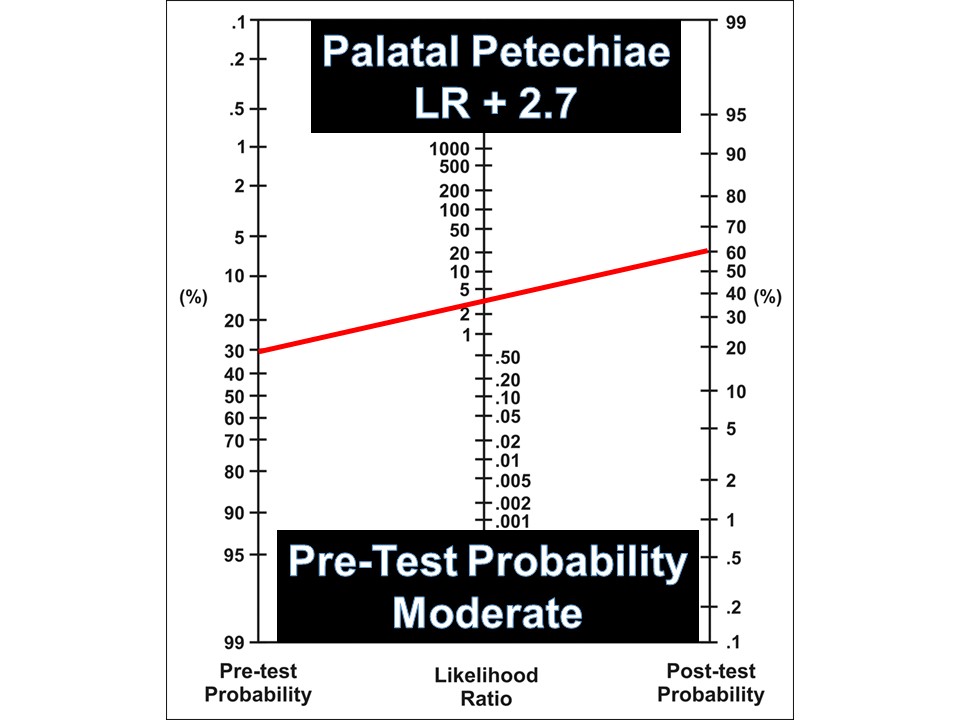
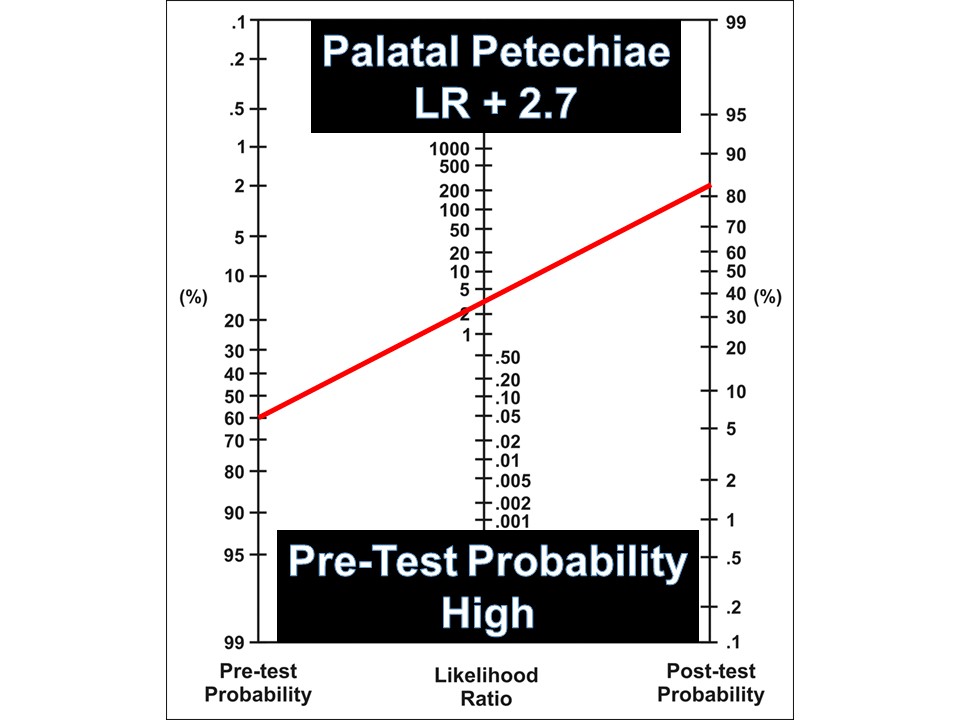
1. Decide on your pre-test probability of the disease (choose an approximate probability based on our assessment)
2. Use the likelihood ratio that correlates to your exam.
3. Draw a straight line frm your pre-test probability starting point, to the LR of the feauture/test, take it through to find your post-test probability
4. Use this new post-test probability to help in your decision
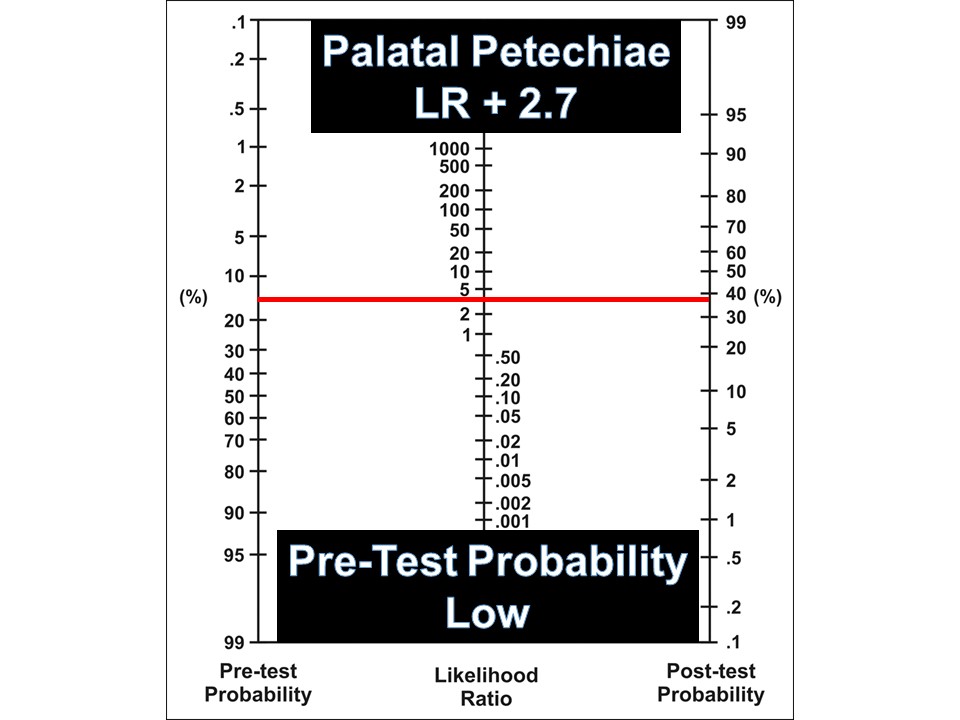
Your patient has palatal petechiae, which confers a positive likelihood ratio (LR+) of 2.7
See below how to use this statistic based on your clinical assessment"
Symptoms and signs | Positive LR (95% CI) | Negative LR (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) |
Scarlatiniform rash | 3.91 (2.00-7.62) | 0.94 (0.90-0.97) | 0.08 (0.05-0.14) | 0.98 (0.95-0.99) |
Palatal petechiae | 2.69 (1.92-3.77) | 0.90 (0.86-0.94) | 0.15 (0.10-0.21) | 0.95 (0.91-0.97) |
Chills | 2.16 (0.94-4.96) | 0.88 (0.79-0.98) | 0.21 (0.18-0.24) | 0.90 (0.83-0.97) |
Anorexia | 1.98 (0.83-4.75) | 0.53 (0.26-1.10) | 0.62 (0.12-1.11) | 0.62 (0.12-1.12) |
Pharyngeal exudate | 1.85 (1.58-2.16) | 0.78 (0.74-0.82) | 0.38 (0.32-0.44) | 0.79 (0.73-0.84) |
Vomiting | 1.79 (1.56-2.06) | 0.85 (0.81-0.90) | 0.28 (0.21-0.36) | 0.84 (0.79-0.89) |
Tender cervical nodes | 1.72 (1.54-1.93) | 0.78 (0.75-0.81) | 0.40 (0.35-0.46) | 0.77 (0.71-0.82) |
Sibling with sore throat | 1.71 (0.82-3.53) | 0.92 (0.82-1.03) | 0.18 (0.14-0.23) | 0.89 (0.83-0.94) |
Halitosis | 1.54 (0.79-2.99) | 0.95 (0.81-1.12) | 0.12 (0.05-0.29) | 0.92 (0.86-0.99) |
Tonsillar and/or pharyngeal exudate | 1.40 (1.10-1.77) | 0.86 (0.75-0.98) | 0.37 (0.28-0.46) | 0.74 (0.68-0.78) |
Large cervical nodes | 1.39 (1.16-1.67) | 0.67 (0.53-0.84) | 0.64 (0.50-0.76) | 0.54 (0.41-0.67) |
Lack of cough | 1.36 (1.18-1.56) | 0.59 (0.48-0.73) | 0.73 (0.66-0.78) | 0.46 (0.38-0.55) |
Tonsillar exudates | 1.35 (0.98-1.87) | 0.81 (0.63-1.06) | 0.46 (0.27-0.67) | 0.66 (0.48-0.80) |
Tonsillar swelling | 1.27 (1.04-1.54) | 0.67 (0.52-0.85) | 0.70 (0.64-0.76) | 0.44 (0.32-0.57) |
Dysphagia | 1.22 (1.00-1.48) | 0.68 (0.51-0.91) | 0.72 (0.55-0.85) | 0.41 (0.23-0.62) |
Headache | 1.22 (0.95-1.57) | 0.90 (0.77-1.04) | 0.39 (0.28-0.51) | 0.68 (0.58-0.76) |
Lack of coryza | 1.21 (1.08-1.35) | 0.69 (0.55-0.88) | 0.72 (0.64-0.79) | 0.40 (0.34-0.48) |
Abdominal pain | 1.18 (0.92-1.51) | 0.95 (0.89-1.03) | 0.24 (0.19-0.30) | 0.79 (0.75-0.83) |
Red tonsils and/or pharynx | 1.13 (0.96-1.33) | 0.41 (0.16-1.02) | 0.93 (0.85-0.96) | 0.18 (0.09-0.35) |
Reported fever | 1.07 (0.96-1.19) | 0.86 (0.67-1.11) | 0.71 (0.58-0.82) | 0.33 (0.23-0.49) |
Red tonsils | 1.07 (0.86-1.34) | 0.82 (0.40-1.69) | 0.80 (0.60-1.00) | 0.25 (0.00-0.51) |
Red pharynx | 1.06 (0.95-1.18) | 0.56 (0.27-1.17) | 0.93 (0.81-0.98) | 0.12 (0.03-0.34) |
Documented temperature >38° or >38.5°C | 1.02 (0.87-1.21) | 0.98 (0.83-1.15) | 0.50 (0.36-0.63) | 0.51 (0.38-0.65) |
Summer | 0.86 (0.61-1.20) | 1.02 (1.00-1.05) | 0.13 (0.00-0.33) | 0.85 (0.65-1.04) |
Arthralgia | 0.74 (0.18-3.08) | 1.02 (0.97-1.06) | 0.09 (0.00-0.25) | 0.90 (0.77-1.04) |
Conjunctivitis | 0.73 (0.46-1.16) | 1.02 (0.98-1.05) | 0.05 (0.02-0.11) | 0.94 (0.85-0.98) |
Acute otitis media | 0.65 (0.14-2.91) | 1.04 (0.93-1.16) | 0.03 (0.01-0.05) | 0.94 (0.84-1.04) |
History of tonsillectomy | 0.64 (0.49-0.84) | 1.07 (1.03-1.11) | 0.11 (0.08-0.13) | 0.84 (0.81-0.86) |
Hoarseness | 0.62 (0.46-0.83) | 1.04 (1.03-1.06) | 0.06 (0.03-0.12) | 0.90 (0.85-0.93) |
Diarrhea | 0.51 (0.33-0.79) | 1.04 (0.99-1.11) | 0.03 (0.00-0.06) | 0.93 (0.86 |
Modified from: Shaikh et al. 2012
This post and podcast are dedicated to Sarah Werner for her constant encouragement of the story in all of us. Check out Write Now with Sarah Werner.
Selected References
Cheung L et al. Throat swab have no influence on the management of patients with sore throats. J Laryngol. 217; 131:977-981.
Ebell MH et al. Rational Clinical Examination: Does This Patient Have Streptococcal Pharyngitis? JAMA. 2000;284(22):2912-2918
Homme JH et al. Duration of Group A Streptococcus PCR positivity following antibiotic treatment of pharyngitis. Diagn Microbiol Infect Dis. 2018 Feb;90(2):105-108.
Nakhoul GN et al. Management of Adults with Acute Streptococcal Pharyngitis: Minimal Value for Backup Strep Testing and Overuse of Antibiotics. J Gen Intern Med. 2013 Jun; 28(6): 830–834.
Oliver J et al. Group A Streptococcus pharyngitis and pharyngeal carriage: A meta-analysis. PLoS Negl Trop Dis. 2018 Mar 19;12(3):e0006335.
Shaikh N, Leonard E, Martin JM. Prevalence of streptococcal pharyngitis and streptococcal carriage in children: a meta-analysis. Pediatrics. 2010 Sep;126(3):e557-64.
Shaikh et al. Accuracy and Precision of the Signs and Symptoms of Streptococcal Pharyngitis in Children: A Systematic Review. J Pediatrics. 2012; 3:487-493.e3
Concussion in Sport Group Guidelines
Concussion Recognition Tool (for coaches, trainers on field)
Child Sports Concussion Assessment Tool, 5th Ed. (Child SCAT); Ages 5-12
Sports Concussion Assessment Tool, 5th Ed. (SCAT5); Ages 13 and Up
This post and podcast are dedicated to the great K Kay Moody, DO, MPH for her stalwart effort to care for both patient and doctor. Thank you for all that you do to help us to be our best and for promoting #FOAMed #FOAMped and #MedEd.
References
Churchill NW et al. The first week after concussion: Blood flow, brain function and white matter microstructure. Neuroimage Clin. 2017; 14: 480–489.
Ellis MJ et al. Psychiatric outcomes after pediatric sports-related concussion. J Neurosurg Pediatr. 2015; 16:709-718.
Graham R et al. and the Committee on Sports-Related Concussions in Youth; Board on Children, Youth, and Families; Institute of Medicine; National Research Council. Sports-Related Concussions in Youth: Improving the Science, Changing the Culture. Washington (DC): National Academies Press (US); 2014 Feb 4.
Harmon KG et al. American Medical Society for Sports Medicine position statement: concussion in sport. Br J Sports Med. 2013; 47:15-26.
McCrory P et al. Consensus statement on concussion in sport—the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med. 2016
Purcell LK et al. What factors must be considered in “return to school” following concussion and what strategies or accommodations should be followed? Br J Sports Med. 2018; 0:1-15.
Wang KK et al. An update on diagnostic and prognostic biomarkers for traumatic brain injury. Exp Rev Molec Gen. 2018; 18(2):165-180.
Wang Y et al. Cerebral Blood Flow Alterations in Acute Sport-Related Concussion. J Neurotrauma. 2016 Jul 1; 33(13): 1227–1236.


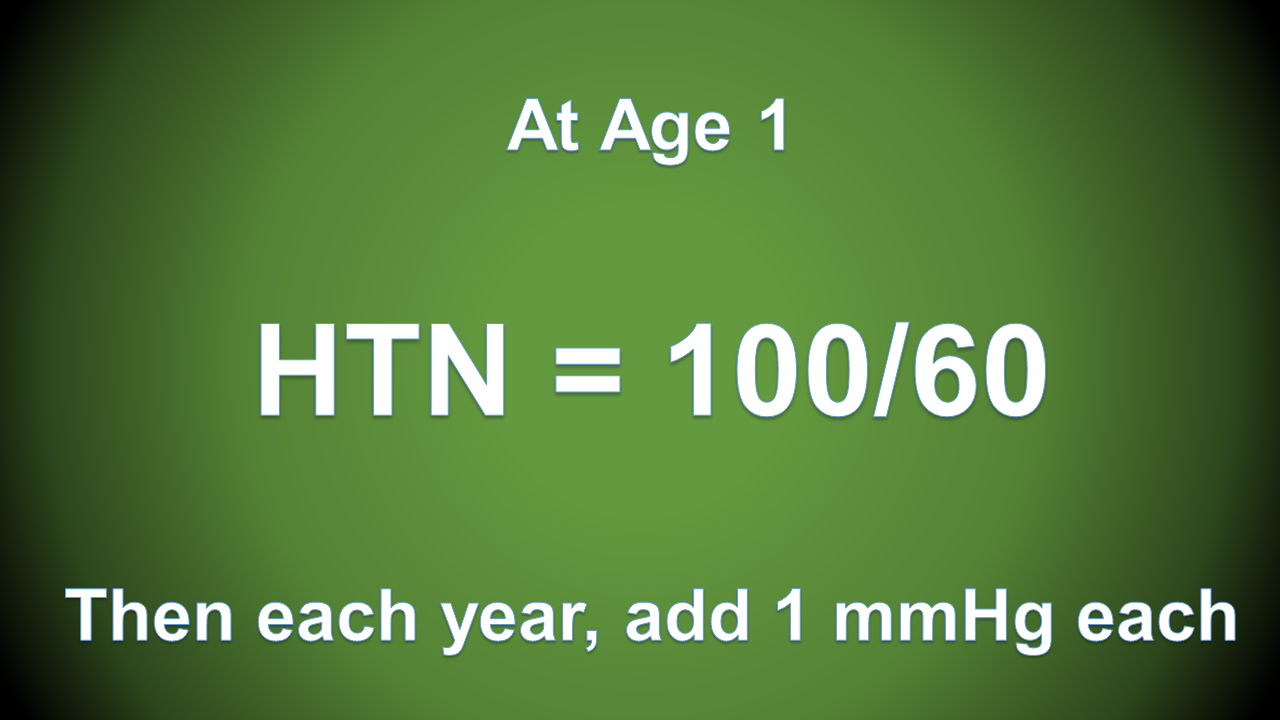
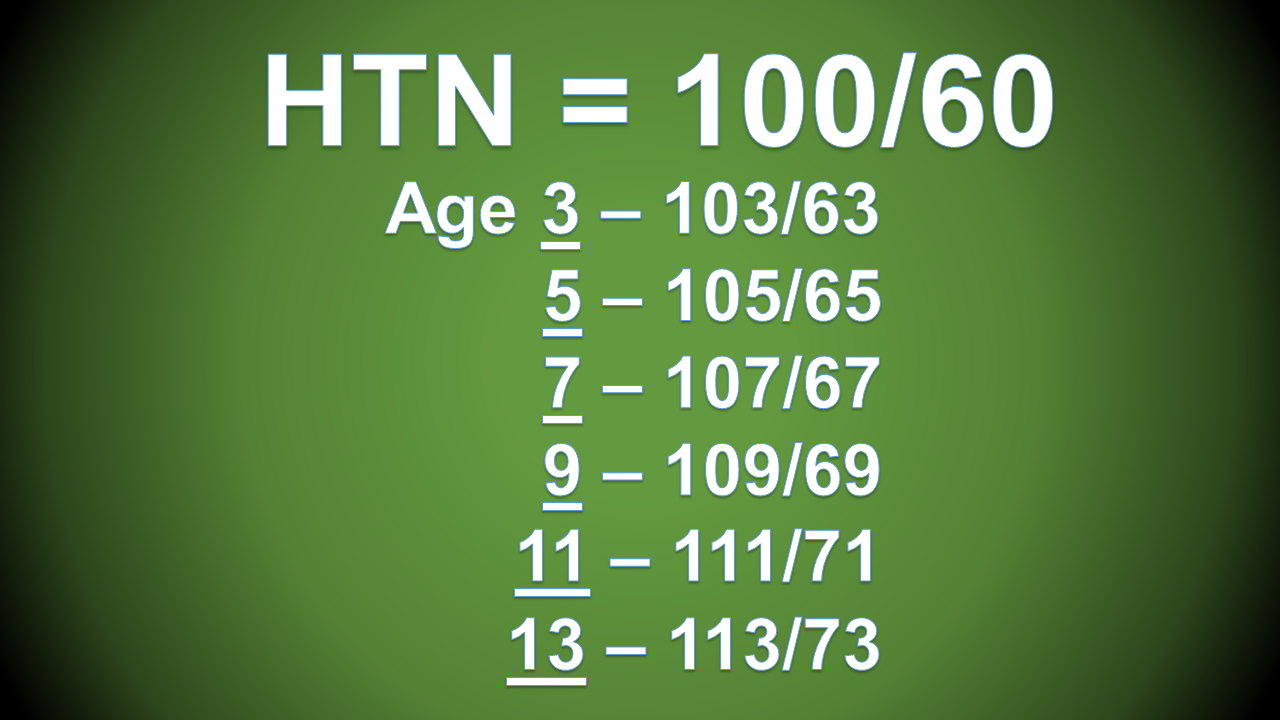




















Baracco R et al. Pediatric Hypertensive Emergencies. Curr Hypertens Rep. 2014; 16:456.
Belsha CW. Pediatric Hypertension in the Emergency Department. Ann Emerg Med. 2008; 51(3):21-24.
Chandar J et al. Hypertensive crisis in children. Pediatr Nephrol. 2012; 27:741-751.
Dionne JM et al. Hypertension Canada’s 2017 Guidelines for the Diagnosis, Assessment, Prevention, and Treatment of Pediatric Hypertension. Canadian J Cardiol. 2017; 33:577-585
*Flynn JT, Kaelber DC, Baker-Smith CM, et al; SUBCOMMITTEE ON SCREENING AND MANAGEMENT OF HIGH BLOOD PRESSURE IN CHILDREN. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics. 2017; 140(3):e20171904
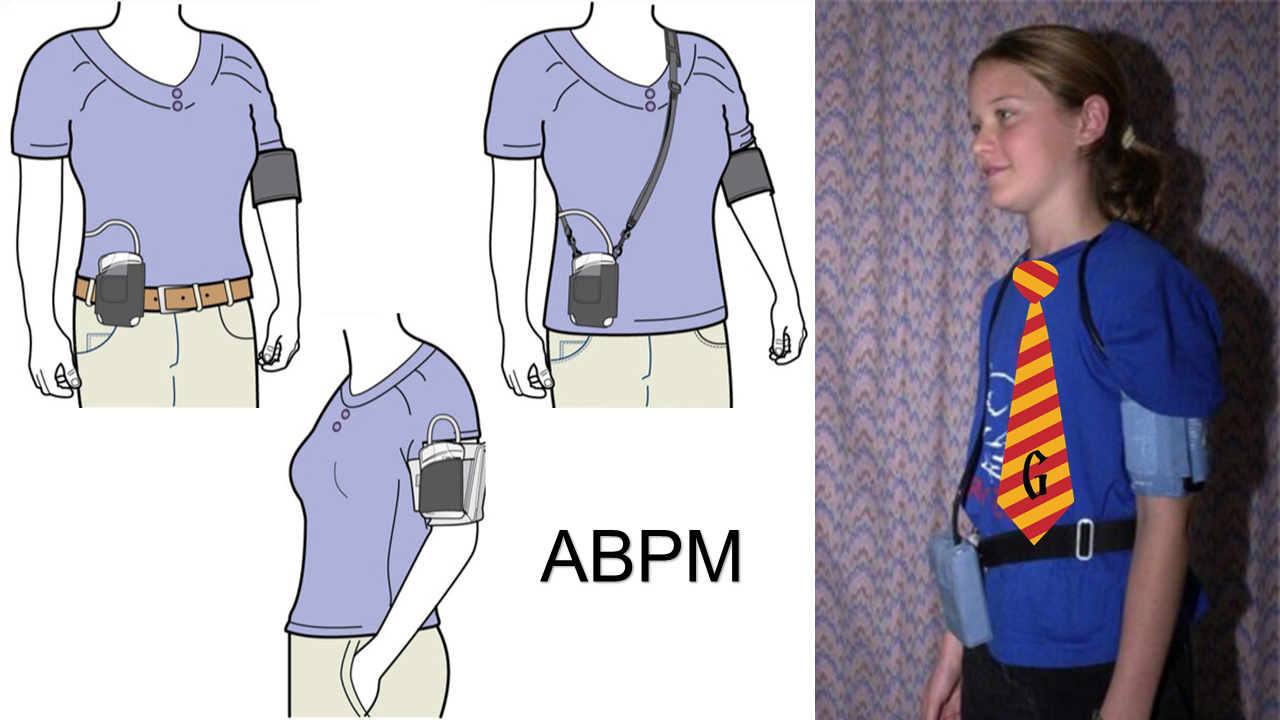
Gilhotra Y et al. Blood pressure measurements on children in the emergency department. Emergency Medicine Australasia. 2006; 18:148-154.
Lurbe E et al. 2016 European Society of Hypertension guidelines for the management of high blood pressure in children and adolescents. J Hypertens. 2016; 34:1-35.
Patel NH et al. Evaluation and management of pediatric hypertensive crises: hypertensive urgency and hypertensive emergencies. Open Access Emergency Medicine. 2012; 4:85-92.
Yang WC et al. Clinical Analysis of Hypertension in Children Admitted to the Emergency Department. Pediatr Neonatol. 2010; 1:44-51.
| Infant to Toddler | Preschool to School Age | Adolescent to Adult |
| Renal disease | Renal disease | Primary hypertension |
| Coarctation of the aorta | Coarctation of the aorta | Medication non-adherence |
| Bronchopulmonary dysplasia | Drug induced/toxicologic | Renal disease |
| Increased intracranial pressure | Increased intracranial pressure | Increased intracranial pressure |
| Volume overload | Pheochromocytoma | Pheochromocytoma |
| Congenital adrenal hyperplasia | Primary hypertension | Drug induced/toxicologic |
Adapted from: Constantine E. Hypertension. In: Textbook of Pediatric Emergency Medicine, 6th Ed. Fleischer GR, Ludwig S, Henretig FM (Eds). Lippincott, Williams & Wilkins, Philadelphia. 2010; p315.
This post and podcast are dedicated to Manpreet 'Manny' Singh for his collegiality, collaboration, and overall awesomeness.
[Details in Audio]















This post and podcast are dedicated to Henry Goldstein, B.Pharm, MBBS for his tireless dedication to all things #FOAMed, #FOAMped, and #MedEd. You are awesome. Make sure to visit Don't Forget the Bubbles!
References
Cohen GM, Albertini LW. Colic. Pediatr Rev. 2012; 33(7):332-3.
Friedman SB et al. The crying infant: diagnostic testing and frequency of serious underlying disease. Pediatrics. 2009; 123(3):841-8
Herman M, Le A. The crying infant. Emerg Med Clin North Am. 2007 Nov;25(4):1137-59.
Poole SR. The infant with acute, unexplained, excessive crying. Pediatrics. 1991; 88 (3): 450-5.
Prentiss KA, Dorfman DH. Pediatric Opthalmology in the Emergency Department. Emerg. Med. Clin. N. Am. 2008; 26: 181-198.
Shope TR, Rieg TS, Kathiria NN. Corneal abrasions in young infants. Pediatrics. 2010 Mar;125(3):e565-9. Epub 2010 Feb 8.



This post and podcast are dedicated to Mads Astvad for sharing his enthusiasm, clinical excellence, and #FOAMed warrior spirit.
Tak, min ven! #SMACConia #Vikingeblod
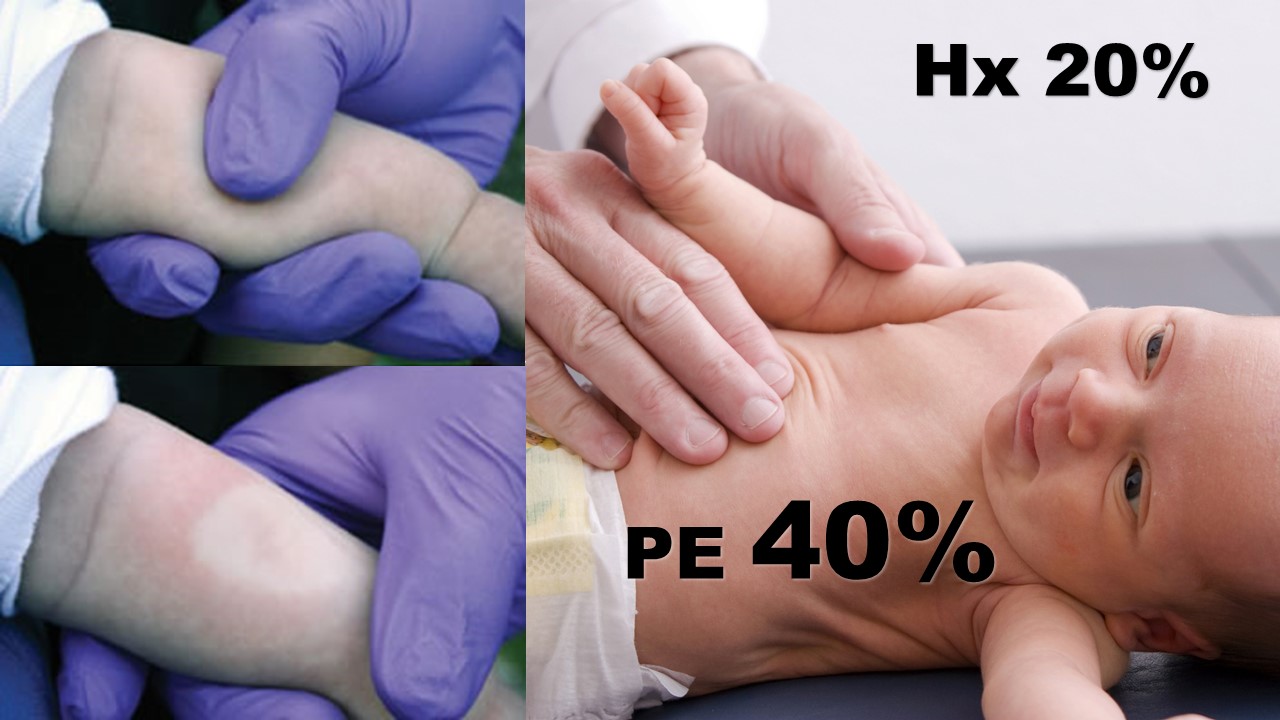
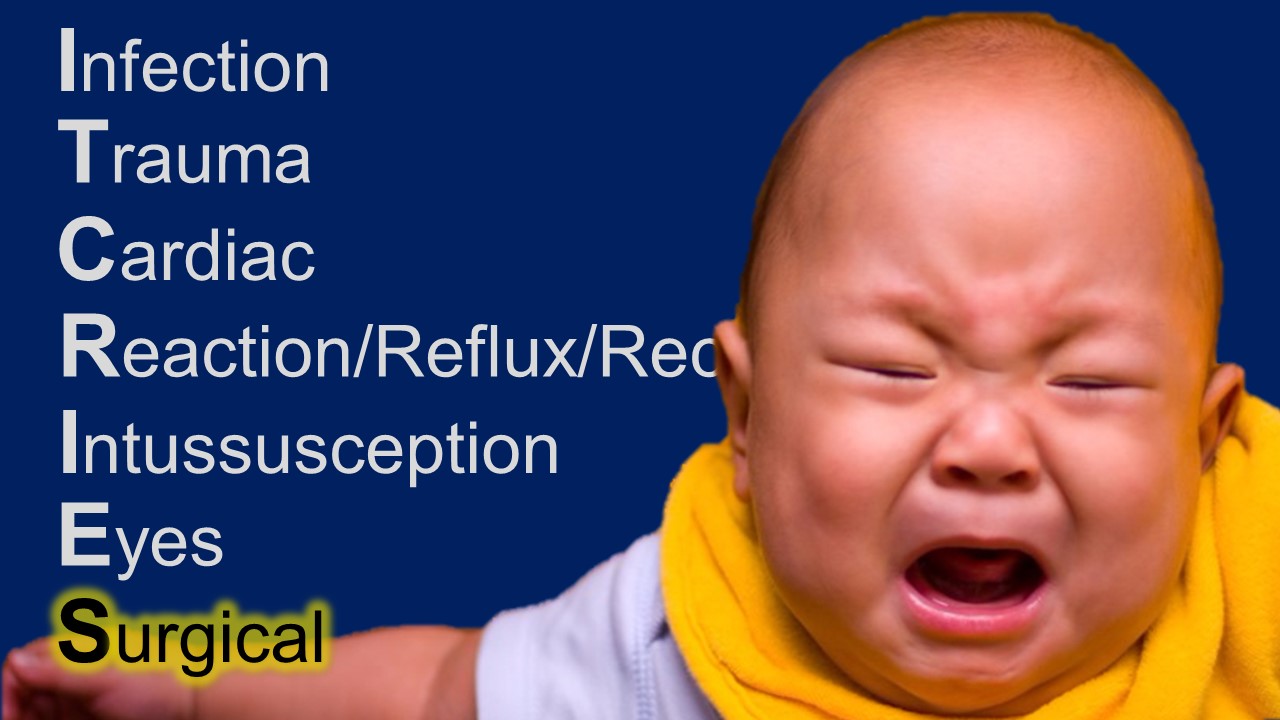
There is none. The presentation varies so much, we need a rule to live by:
Unilateral pelvic pain in a girl is ovarian torsion until proven otherwise. This includes the cases in which you are concerned about appendicitis. They both can be fake-outs.
Often the pain is severe and abrupt, but trying to tease this out is often not fruitful.
Here are the often-reported signs and symptoms associated with ovarian torsion:
Stabbing pain, 70%
Nausea and vomiting, 70%
Sudden, sharp pain in the lower abdomen, 59%
Pain radiating to the back, flank, or groin, 51%
Peritoneal signs, 3%
Fever, less than 2%
And of course…no pain on presentation…30%...intermittent torsion.
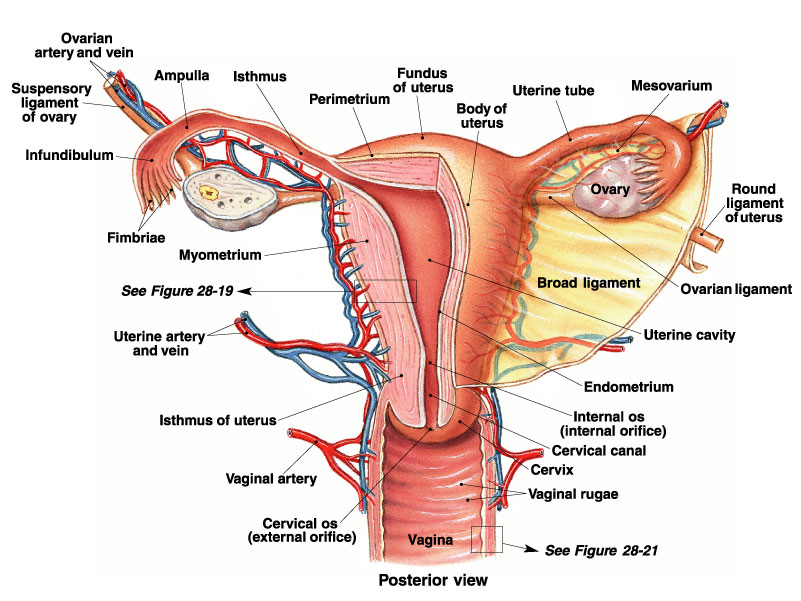
As far as Doppler flow goes, you may see one of several scenarios:
Other things you may see on ultrasound include focal tenderness with the probe, or the whirlpool sign – this is a twisted vascular pedicle.
In children, is there an ovarian size (volume) that rules out torsion?”
In the Journal of Pediatric Radiology, Servaes et al catalogued the ultrasound findings in children with surgically confirmed torsion over a 12 year period. In this case series of 41 patients, the median age was 11. The age range was one month old to 21 years of age. They found that in torsed ovaries, the ovarian volume was 12 x that compared to the normal, non-torsed contralateral ovary.
That is to say, in this case series all torsed ovaries were larger than the normal contralateral ovary.
Sudden unilateral lower abdominal or pelvic pain in a female? Think torsion.
Have a low threshold for investigation.
Know the performance characteristics of ultrasound findings and involve a gynecologist early.
This post and podcast are dedicated to Stephanie Doniger, MD for her enthusiasm, spirit, and expertise in #MedEd #FOAMed #FOAMped #POCUS
Abe M, Sarihan H. Oophoropexy in children with ovarian torsion. Eur. J. Pediatr. Surg. 2004;14:168.
Aziz D, Davis V, Allen L, Langer J. Ovarian torsion in children: Is oophorectomy necessary? J. Pediatr. Surg. 2004;39:750-3.
Bristow RE, Nugent AC, Zahurak ML, et al. Impact of surgeon specialty on ovarian-conserving surgery in young females with an adnexal mass. J. Adolesc. Health 2006;39:411.
Chang YJ, Yan DC, Kong MS, et al. Adnexal torsion in children. Pediatr. Emerg. Care. 2008;24:534-7.
Conforti A, Giorlandino C, Bagolan P. Fetal ovarian cysts management and ovarian prognosis: a report of 82 cases. J. Pediatr. Surg. 2009;44:868; author reply 868-9.
Guthrie BD, Adler MD, Powell EC. Incidence and trends of pediatric ovarian torsion hospitalizations in the United States, 2000-2006. Pediatrics 2010;125:532-8. Epub 2010 Feb 1.
Houry D, Abbott JT. Ovarian torsion: a fifteen-year review. Ann. Emerg. Med. 2001;38:156-9.
Huang TY, Lau BH, Lin LW, Wang TL, Chong CF, Chen CC. Ovarian cyst torsion in a toddler. Am. J. Emerg. Med. 2009;27:632, e1-3.
Hurh PJ, Meyer JS, Shaaban A. Ultrasound of a torsed ovary: characteristic gray-scale appearance despite normal arterial and venous flow on Doppler. Pediatr. Radiol. 2002;32:586-8. Epub 2002 May 25.
Kokoska E, Keller M, Weber T. Acute ovarian torsion in children. Am. J. Surg. 2000;180:462-5.
Oltmann SC, Fischer A, Barber R, Huang R, Hicks B, Garcia N. Cannot exclude torsion – a 15-year review. J. Pediatr. Surg. 2009;44:1212-6; discussion 1217.
Chmitt ER et al. Twist and Shout! Pediatric Ovarian Torsion Clinical Update and Case Discussion. Pediatr Emerg Care. 2013; 29(4):518-523.
Servaes S, Zurakowski D, Laufer MR, Feins N, Chow JS. Sonographic findings of ovarian torsion in children. Pediatr. Radiol. 2007;37:446-51. Epub 2007 Mar 15.
Valsky DV. Added value of the gray-scale whirlpool sign in the diagnosis of adnexal torsion. Ultrasound Obstet. Gynecol. 2010;36:630-4.
Normally metabolized into codeine-6-glucuronide (50-70%) and norcodeine (10-15%). Codeine, codeine-6-glucuronide, and norcodeine have low affinity for the μ (mu) receptor.
However, the most active metabolite of codeine is morphine with 200x the affinity for the mu receptor as the codeine derivates. The problem is, people vary in its metabolism from 0-15% of codeine is metabolized to morphine.
Ok, codeine is lame at best, unpredictable at worst.
True. Unless you are hiding a genetic time bomb.
You're an ultra-rapid metabolizer.
Some people have multiple extra copies of the DNA sequence for the CYP2D6 enzyme. Ultra rapid metabolizers funnel a huge proportion of their codeine into morphine metabolism, resulting in a bolus of morphine, ending in apnea.
This combination is no better than placebo -- all of the risks, with no proven benefit. This combination is notoriously abused -- as purple drank or sizzurp. The rapper Pimp C died of this.
Speaking of cough syrups...
The AAP recommends no cough and cold preparations in children under age 6. They have not been adequately studied in young children, and are not recommended for treating the common cold.
What then? You gotta give me something, doctor!
Ok, Honey!
In a study in the Archives of Pediatric and Adolescent Medicine, Dr Paul and colleagues published: Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents. They compared a buckwheat honey, honey-flavored dextromethorphan (DM) and no treatment 30 min before bed for children with upper respiratory tract infections.
Of the three, honey, dextromethorphan, and no treatment – honey scored the best for symptom improvement and cough frequency.
Over age 1? Cough and cold? Honey. There is no concern about accidental overdose, parents are doing something with a proven effect, and compliance is pretty much 100% -- and Grandma approves.
No proven benefit over placebo. Also widely abused, in pill form ("Skittles") and/or liquid form mixed in alcoholic beverage ("robotripping").
Allow the child to speak for himself whenever possible. After acknowledging the parent’s input, perhaps try “I want to make sure I understand how the pain is for you. Tell me more.”
Engage parents and communicate the plan to them. Elicit their expectations, and give them of preview of what to expect in the ED.
Opioids are meant for pain caused by acute tissue injury, for the briefest period of time feasible. Older school-aged children and adolescents are increasingly at risk for opioid dependence and addiction.
Give detailed advice on how to manage pain at home. Set expectations. Let them know you understand and will help them through your good advice that will carry them through this difficult time. Patients and families often just need a plan. Map it out clearly.
And...
Just say no to: codeine, promethazine with codeine, and dextramethorphan.
FDA. Most Young Children With a Cough or Cold Don't Need Medicine.
Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet. 2004;43(13):879-923.
This post and podcast are dedicated to Bryan Hayes, PharmD for his practical approach to pharmacologic conundrums and to David Juurlink, MD, PhD for his steadfast dedication to patient safety and clinician education. Check out Bryan's helpful blog and clinical resource, PharmERToxGuy. Check out David anywhere one utters the word Tra-ma-dol.
This post and podcast are dedicated to Kevin Klauer, DO, EJD, FACEP for his dedication to education, and for his unique balance of safety and keeping it real. Thank you.
For intractable epilepsy; sends retrograde signal up corona radiata
Also may be used in: depression, bulimia, Alzheimer, narcolepsy, addiction, and others


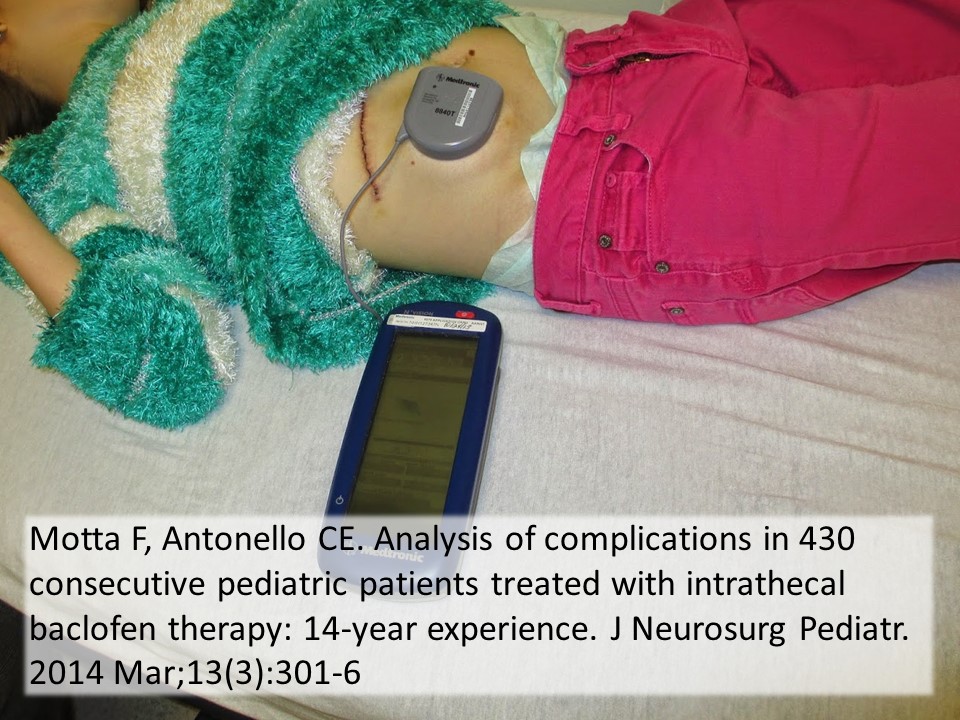
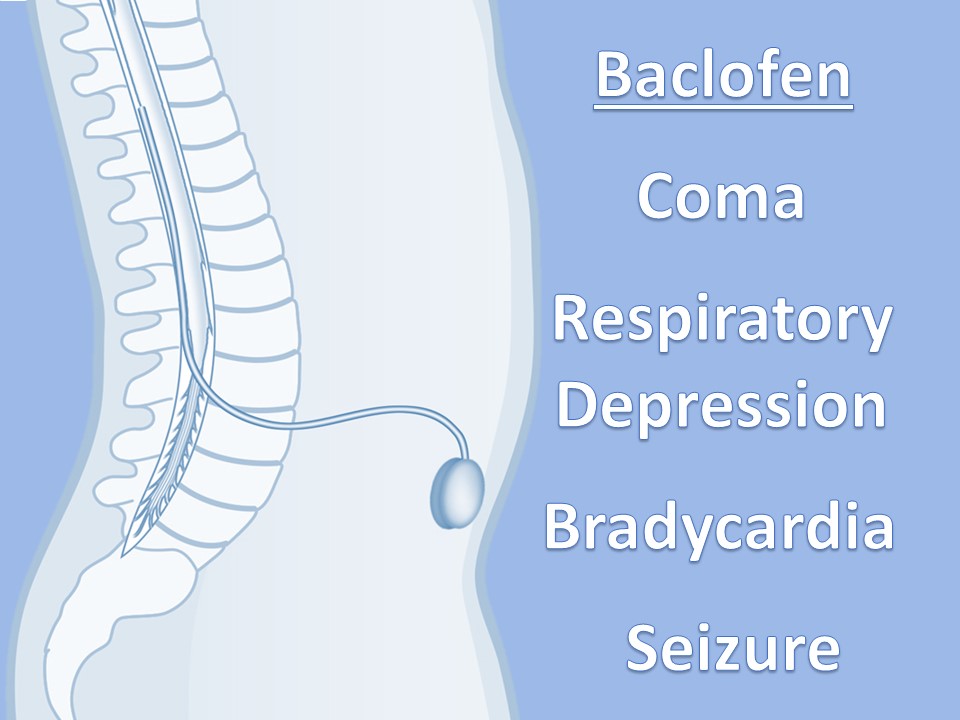
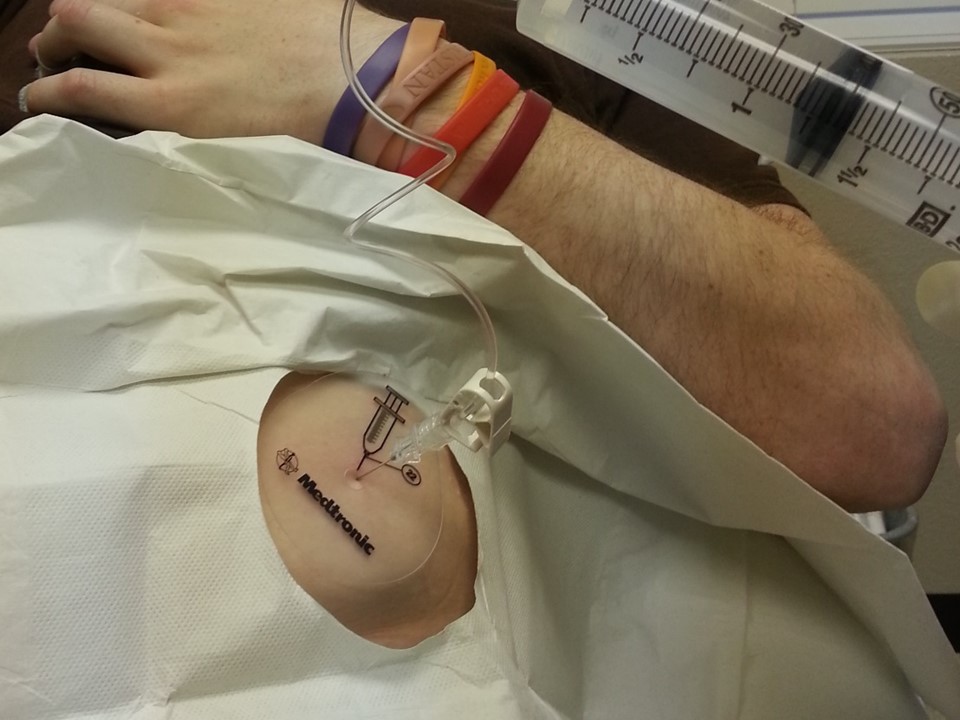
Used to infuse basal rate of drug, usually baclofen for spasticity, but pump may contain morphine, bupivicaine, clonidine. Also used for severe MS, stroke, TBI, chronic pain. Verify the medication and identify the toxidrome if symptomatic.




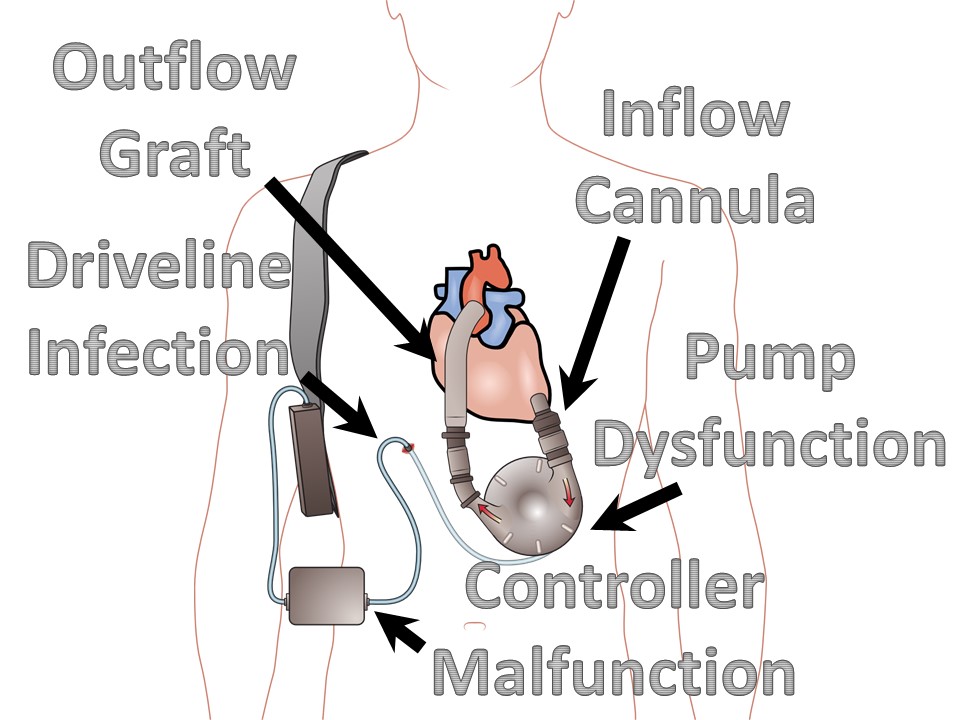
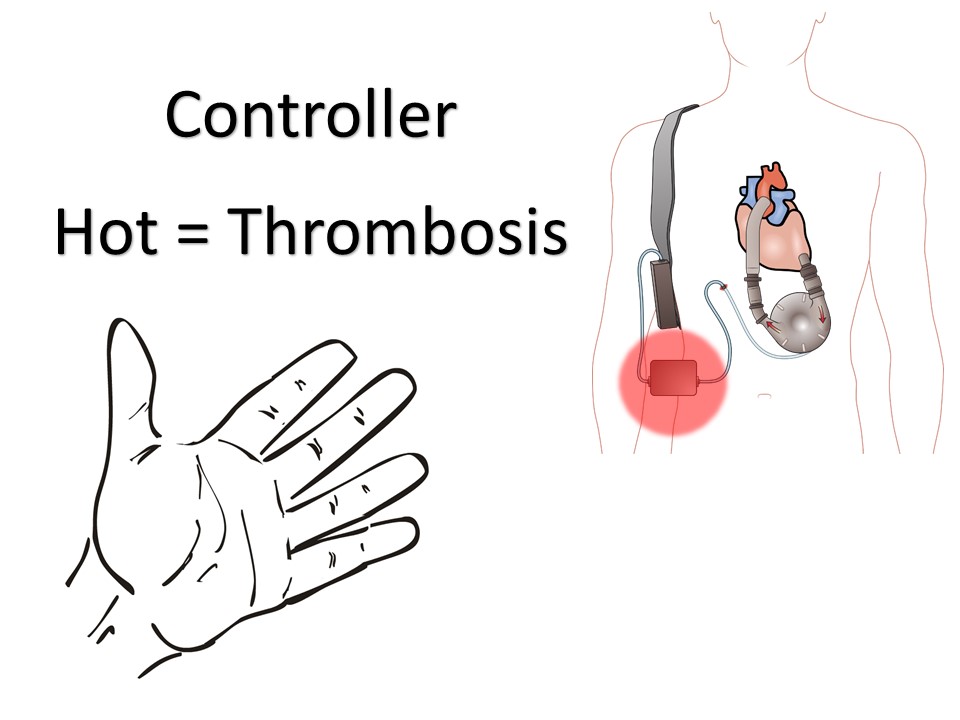
May be left ventricular assist, right ventricular assist, or biventricular assist device.


Elliott RE, Rodgers SD, Bassani L et al. Vagus nerve stimulation for children with treatment-resistant epilepsy: a consecutive series of 141 cases. J Neurosurg Pediatrics. 2011; 7:491-500.
Groves DA, Brown VJ. Vagal nerve stimulation: a review of its applications and potential mechanisms that mediate its clinical effects. Neuroscience and Biobehavioral Reviews. 2005; 29: 493–500.
Panebianco M, Rigby A,Weston J,Marson AG. Vagus nerve stimulation for partial seizures. Cochrane Database of Systematic Reviews. 2015; 4, Art. No.: CD002896.
Ruffoli R, Giorgi FS, Pizzanelli C et al. The chemical neuroanatomy of vagus nerve stimulation. Journal of Chemical Neuroanatomy; 2011; 42: 288–296.
Borowski A, Littleton AG, Borkhuu B et al. Complications of Intrathecal Baclofen Pump Therapy in Pediatric Patients. J Pediatr Orthop. 2010; 30:76–81.
Ghosh D, Mainali G, Khera J, Luciano M. Complications of Intrathecal Baclofen Pumps in Children: Experience from a Tertiary Care Center. Pediatr Neurosurg. 2013; 49:138–144.
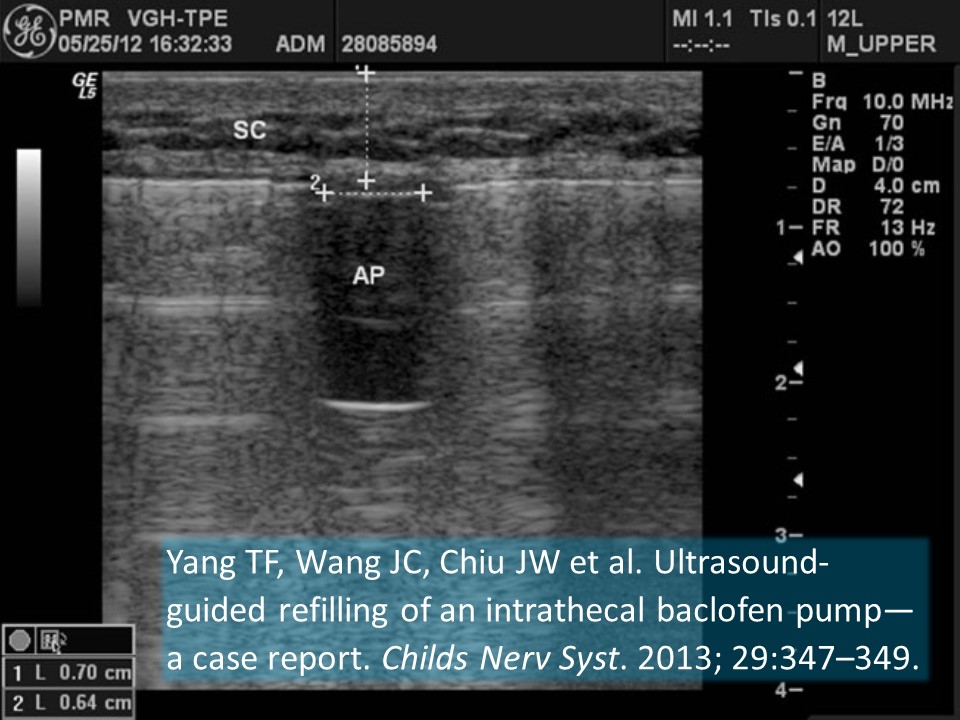
Yang TF, Wang JC, Chiu JW et al. Ultrasound-guided refilling of an intrathecal baclofen pump—a case report. Childs Nerv Syst. 2013; 29:347–349.
Yeh RN, Nypaver MM, Deegan TJ, Ayyangar R. Baclofen Toxicity in an 8-year-old with an Intrathecal Baclofen Pump. J Emerg Med. 2004; 26(4): 163–167.
Blume ED, Naftel DC, Bastardi HJ et al. for the Pediatric Heart Transplant Study Investigators. Outcomes of Children Bridged to Heart Transplantation With Ventricular Assist Devices: A Multi-Institutional Study. Circulation. 2006; 113: 2313-2319.
Colón JE, Laborde ME, Nossaman BD. Case Report: Left Ventricular Assist Device in a 12 Year Old Child as a Bridge to Heart Transplantation. Section of Congenital Cardiac Anesthesia, Ochsner Medical Center, New Orleans, Louisiana. 2012.
Fan Y, Weng YG, Huebler M et al. Predictors of In-Hospital Mortality in Children After Long-Term Ventricular Assist Device Insertion. J Amer Coll Cardiol. 2011; 58(11):1183–90
Fraser CD, Jaquiss RDB, Rosenthal DN et al. Prospective Trial of a Pediatric Ventricular Assist Device. N Engl J Med. 2012;367:532-41.
Gazit AZ, Gandhi SK, Canter CC. Mechanical Circulatory Support of the Critically Ill Child Awaiting Heart Transplantation. Current Cardiology Reviews. 2010; 6: 46-53.
VanderPluym CJ, Fynn-Thompson F, Blume ED. Ventricular Assist Devices in Children Progress With an Orphan Device Application. Circulation. 2014;129:1530-1537.
This post and podcast are dedicated to Joe Bellezzo, MD, FACEP and Zack Shinar, MD, FACEP for bringing us all up to speed. Listen to their fantastic ED ECMO podcast here.